Hiroshima and Nagasaki Death Toll
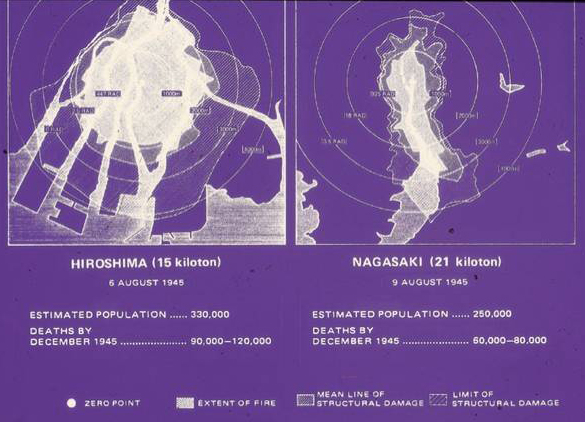
The mortality was greater in Hiroshima because the city was located in a flat delta, in contrast to Nagaskis Urakami Valley. The Nagasaki-Urakami is enclosed by mountain ridges that shielded the city. Nevertheless, the instant lethal effect revealed consideration of the use of these annhilative weapons in warfare can be tolerated by man now that nukes of far greater destructive power are now available.
The real mortality of the atomic bombs that were dropped on Japan will never be known. The destruction and overwhelming chaos made orderly counting impossible. It is not unlikely that the estimates of killed and wounded in Hiroshima (150,000) and Nagasaki (75,000) are over conservative.
At no time during the period between 1943 and 1946 were facilities allotted, or time provided, for the Medical Section of the Manhattan Engineer District to prepare a comprehensive history of its activities. Regulations forbade notetaking. Official records were scanty. There were few charts and photographs.
Atomic attack death toll.
From their own observations and from testimony of Japanese, members of the survey team divided the morbidity and mortality of the atomic bombs that were dropped on Japan into the following phases:
- Very large numbers of person were crushed in their homes and in the buildings in which they were working. Their skeletons could be seen in the debris and ashes for almost 1,500 meters from the center of the blast, particularly in the downwind directions.
- Large numbers of the population walked for considerable distances after the detonation before they collapsed and died.
- Large numbers developed vomiting and bloody and watery diarrhea (vomitus and bloody fecees were found on the floor in many of the aid stations), associated with extreme weakness. They died in the first and second weeks after the bombs were dropped.
- During this same period deaths from internal injuries and from burns were common. Either the ehat from the fires or infrared radiation from the detonations caused many burns, particularly on bare skin or under dark clothing.
- After a lull without peak mortality from any special causes, deaths began to occur from purpura, which was often associated with epilation, anemia, and a yellowish coloration of the skin. The so-called bone marrow syndrome, manifested by a low white blood cell count and almost complete absence of the platelets necessary to prevent bleeding,w as probably at its maximum beTween the fourth and sixth weeks after the bombs were dropped.
